Attention personal trainers!!!
Quiz of the day: What primary muscle is required to assist with slowing down the thigh when descending stairs?
a. concentric gastrocnemius muscle
b. eccentric anterior tibialis muscle
c. eccentric quadricep
d. neutral quadratus lumborum muscle
To win a free home study course, please email your answer to: ptcg1999@verizon.net
www.pinnacle-tcs.com
"Teaching The Science Behind The Movement"
Thursday, May 21, 2020
Tip of the Day
By Chris Gellert, PT, MMusc & Sportsphysio, MPT, CSCS, C-IASTMPinnacle Training. & Consulting Systems, LLC
During these tough and uncertain times, it is important to reflect. There are 5 stages to get anything under control. By practicing and implementing these five stages into your life, this could bring calmness to the storm and clarity to your daily life.
1) Collect collect everything around you and get it ready to be reviewed and organized.
2)Process take the information and look over which should take a few minutes.
3)Organize what you have gathered and this could be creating a list, putting things in folders on your computer or literally folders on your desk.
4)Review-review everything weekly to ensure that you are staying on top of the projects and obligations.
5) Do-Just do it as this should help you make choices about your next actions
Tuesday, May 19, 2020
Wednesday at 12pm eastern time is Chris Gellert, PT who will be taking questions as Aska PT!
A live show where you can ask questions about clients, programming as well as other topics on your mind.
#movement#human movement#manual therapy#manual therapy seminars#PersonalTrainerCEUs #MassageTherapistsCEUs #PhysicalTherapistsCEUs #PhysicalTherapyAssistantsCEUs #OnlineEducation #CEUs #PinnacleTrainingConsultingSystems #PTCS #CapeCod
www.PersonalTrainerCEU.com
www.pinnacle-tcs.com
Monday, May 18, 2020
Top 3 exercises for Lumbar
Spondylosis, Spinal stenosis and Spondylolisthesis
By Chris Gellert, PT, MMusc &
Sportsphysio, MPT, CSCS, C-IASTM
Pinnacle Training & Consulting Systems
Pinnacle Training & Consulting Systems
Background
There are a multitude of exercises
available at the fingertips of a fitness professional. Choosing
the most accurate and objective exercise should be the cornerstone of any fitness
programming. Working with any client who has a spinal injury, should involve a thorough
history, fitness assessment and most importantly, a sound understanding of the pathophysiology
and programming of that movement dysfunction. In this article, we will review and clarify
the differences between spinal conditions that include spondylosis, spinal stenosis and
spondylolisthesis discussing the pathophysiology, common rehabilitation and post
rehabilitation training.
the most accurate and objective exercise should be the cornerstone of any fitness
programming. Working with any client who has a spinal injury, should involve a thorough
history, fitness assessment and most importantly, a sound understanding of the pathophysiology
and programming of that movement dysfunction. In this article, we will review and clarify
the differences between spinal conditions that include spondylosis, spinal stenosis and
spondylolisthesis discussing the pathophysiology, common rehabilitation and post
rehabilitation training.
Clarifying
the differences
Spondylosis
is the degeneration of one joint on another also known as degenerative
disc
disease(DJD). Patient will typically presents with tightness in the lower lumbar and may or may
not present with radicular symptoms in their legs. Physical therapy addresses these impairments
by conducting a comprehensive examination, using manual therapy, and targeted exercises.
disease(DJD). Patient will typically presents with tightness in the lower lumbar and may or may
not present with radicular symptoms in their legs. Physical therapy addresses these impairments
by conducting a comprehensive examination, using manual therapy, and targeted exercises.
 Spinal stenosis is a
narrowing within the vertebral canal
Spinal stenosis is a
narrowing within the vertebral canal coupled with hypertrophy of the spinal lamina and
ligamentum flavum or facets as the result of age-related
degenerative process. The patient who has spinal stenosis
usually has very tight hamstrings and lumbar extensors.
They often will complain of unilateral vs. bilateral numbness in their legs due either having central lateral(to side) foraminal stenosis.
Physical therapy addresses these areas with myofascial
release, stretching, and joint mobilizations to address
mobility then teach flexion based exercises, which will
improve the opening of the spinal lamina.
Figure 1. Spinal stenosis
Spondylolistehsis is an anterior (forward) slippage or
posterior (back) slippage of one vertebrae on another following bilateral
fracture of the pars interarticularis. The slippage is graded from 1-4 (25% to
100%) from an x-ray. In degenerative spondylolisthesis, as the intervertebral
disc loses height, the annulus may bulge circumferentially and the ligamentum
flavum can buckle. These types of injuries are seen in wrestlers, due to the
combined extension and rotation movements seen in the sport as well as in older
patients due to their lifestyle. Physical therapy/training emphasis is on elimination of extension-based
exercise (back extension, press ups, etc.). Biomechanically, this will force
the vertebra forward causing more translation and instability. Training emphasis is on flexion-based exercises (strengthening of
abdominals). Flexion based exercises will decrease shearing force and
translation on the effected segment. Postural education is key, static and
dynamic core strengthening should also be included. Core strengthening using medicine balls, cables and physioballs shoulder
be personalized to the client.
Recommendations
All of the spinal
conditions discussed previously are unique, requiring a thorough understanding,
while designing a program that is personalized for the client. With respect to
spondylosis, the three top exercises for this client are abdominal bracing with
alternate leg lift, bridging with physioball and prone alternate leg lift/arm
lift over physioball. All three exercises target the multifidus and transverse
abdominis. Two essential muscles of the core.


Figure 2. Abdominal bracing with alternate leg lift Figure 3. Prone alternate arm and leg lift
With respect to both spinal stenosis and spondylolisthesis, the focus is on flexion exercises.
My top three for both
include reverse abdominal crunch, dead bug and prone alternate leg and arm lift
over physioball, stopping at neutral(as seen in figure 3).


Figure 4. Reverse crunch
Figure 5. Dead bug
Summary
Lumbar Spondylosis,
Spinal stenosis and Spondylolisthesis are three common spinal conditions
affecting most adults today. Understanding the pathophysiology, mechanism of
injury, common physical therapy treatments and a few targeted exercises, should
help you, the fitness professional while designing a program for your client.
If you should have any questions, please feel free to contact PTCS at ptcg1999@verizon.net or www.pinnacle-tcs.com
Thursday, May 14, 2020
Top 3 exercises for Lumbar Spondylosis, Spinal stenosis and Spondylolisthesis
By Chris Gellert, PT, MMusc & Sportsphysio, MPT, CSCS, C-IASTM
Pinnacle Training & Consulting Systems
Pinnacle Training & Consulting Systems
Background
There are a multitude of exercises available at the fingertips of a fitness professional. Choosing
the most accurate and objective exercise should be the cornerstone of any fitness
programming. Working with any client who has a spinal injury, should involve a thorough
history, fitness assessment and most importantly, a sound understanding of the pathophysiology
and programming of that movement dysfunction. In this article, we will review and clarify
the differences between spinal conditions that include spondylosis, spinal stenosis and
spondylolisthesis discussing the pathophysiology, common rehabilitation and post
rehabilitation training.
the most accurate and objective exercise should be the cornerstone of any fitness
programming. Working with any client who has a spinal injury, should involve a thorough
history, fitness assessment and most importantly, a sound understanding of the pathophysiology
and programming of that movement dysfunction. In this article, we will review and clarify
the differences between spinal conditions that include spondylosis, spinal stenosis and
spondylolisthesis discussing the pathophysiology, common rehabilitation and post
rehabilitation training.
Clarifying the differences
Spondylosis is the degeneration of one joint on another also known as degenerative disc disease(DJD). The patient will typically presents with tightness in the lower lumbar and may or may not present with radicular symptoms in their legs. Physical therapy addresses these impairments
by conducting a comprehensive examination, using manual therapy, and targeted exercises.
by conducting a comprehensive examination, using manual therapy, and targeted exercises.
Spinal stenosis is a narrowing within the vertebral canal coupled with hypertrophy of the
spinal lamina and ligamentum flavum or facets as the result of the age-related degenerative process.
The patient who has spinal stenosis usually has very tight hamstrings and lumbar extensors.
They often will complain of unilateral vs. bilateral numbness in their legs due either having central
lateral(to side) foraminal stenosis. Physical therapy addresses these areas with myofascial release,
stretching, and joint mobilizations to address mobility then teach flexion based exercises which
will improve the opening of the spinal lamina.
spinal lamina and ligamentum flavum or facets as the result of the age-related degenerative process.
The patient who has spinal stenosis usually has very tight hamstrings and lumbar extensors.
They often will complain of unilateral vs. bilateral numbness in their legs due either having central
lateral(to side) foraminal stenosis. Physical therapy addresses these areas with myofascial release,
stretching, and joint mobilizations to address mobility then teach flexion based exercises which
will improve the opening of the spinal lamina.

Figure 1. Spinal stenosis
Spondylolisthesis is an anterior (forward) slippage or posterior (back) slippage of one vertebra on another following bilateral fracture of the pars interarticularis. The slippage is graded from 1-4 (25% to 100%) from an x-ray. In degenerative spondylolisthesis, as the intervertebral disc loses height, the annulus may bulge circumferentially and the ligamentum flavum can buckle. These types of injuries are seen in wrestlers, due to the combined extension and rotation movements seen in the sport as well as in older patients due to their lifestyle. Physical therapy/training emphasis is on the elimination of extension-based exercise (back extension, press-ups, etc.). Biomechanically, this will force the vertebra forward causing more translation and instability. Training emphasis is on flexion-based exercises (strengthening of abdominals). Flexion based exercises will decrease the shearing force and translation on the affected segment. Postural education is key, static and dynamic core strengthening should also be included. Core strengthening using medicine balls, cables, and physioballs shoulder be personalized to the client.
Recommendations
All of the spinal conditions discussed previously are unique, requiring a thorough understanding while designing a program that is personalized for the client. With respect to spondylosis, the three top exercises for this client are abdominal bracing with alternate leg lift, bridging with physioball, and prone alternate leg lift/arm lift over physioball. All three exercises target the multifidus and transverse abdominis. Two essential muscles of the core.
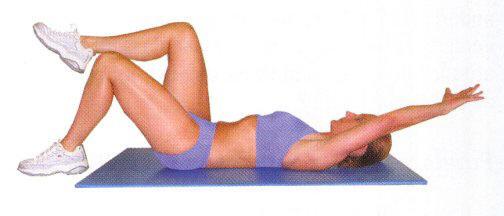

Figure 2. Abdominal bracing with alternate leg lift Figure 3. Prone alternate arm and leg lift
With respect to both spinal stenosis and spondylolisthesis, the focus is on flexion exercises.
My top three for both include reverse abdominal crunch, dead bug, and prone alternate leg and arm lift over physioball, stopping at neutral(as seen in figure 3).


Figure 4. Reverse crunch Figure 5. Dead bug
Summary
Lumbar Spondylosis, Spinal stenosis, and Spondylolisthesis are three common spinal conditions affecting most adults today. Understanding the pathophysiology, mechanism of injury, common physical therapy treatments, and a few targeted exercises, should help you, the fitness professional while designing a program for your client. If you should have any questions, please feel free to contact PTCS at ptcg1999@verizon.net or www.pinnacle-tcs.com
Top 3 exercises for Lumbar Spondylosis, Spinal stenosis and Spondylolisthesis
By Chris Gellert, PT,
MMusc & Sportsphysio, MPT, CSCS, C-IASTM
Pinnacle Training & Consulting Systems
Pinnacle Training & Consulting Systems

Background
There are a multitude of exercises
available at the fingertips of a fitness professional. Choosing
the most accurate and objective exercise should be the cornerstone of any fitness
programming. Working with any client who has a spinal injury, should involve a thorough
history, fitness assessment and most importantly, a sound understanding of the pathophysiology
and programming of that movement dysfunction. In this article, we will review and clarify
the differences between spinal conditions that include spondylosis, spinal stenosis and
spondylolisthesis discussing the pathophysiology, common rehabilitation, and post
rehabilitation training.
the most accurate and objective exercise should be the cornerstone of any fitness
programming. Working with any client who has a spinal injury, should involve a thorough
history, fitness assessment and most importantly, a sound understanding of the pathophysiology
and programming of that movement dysfunction. In this article, we will review and clarify
the differences between spinal conditions that include spondylosis, spinal stenosis and
spondylolisthesis discussing the pathophysiology, common rehabilitation, and post
rehabilitation training.
Clarifying
the differences
Spondylosis
is the degeneration of one joint on another
also known as degenerative disc
disease (DJD). The patient will typically present with tightness in the lower lumbar and may or may
not present with radicular symptoms in their legs. Physical therapy addresses these impairments
by conducting a comprehensive examination, using manual therapy, and targeted exercises.
disease (DJD). The patient will typically present with tightness in the lower lumbar and may or may
not present with radicular symptoms in their legs. Physical therapy addresses these impairments
by conducting a comprehensive examination, using manual therapy, and targeted exercises.
 |
| Spinal Stenosis |
spinal lamina and ligamentum flavum or facets as the result of age-related degenerative process.
The patient who has spinal stenosis usually has very tight hamstrings and lumbar extensors.
They often will complain of unilateral vs. bilateral numbness in their legs due either having central
lateral (to side) foraminal stenosis. Physical therapy addresses these areas with myofascial release,
stretching, and joint mobilizations to address mobility then teach flexion-based exercises which
will improve the opening of the spinal lamina.
Spondylolisthesis is an anterior (forward) slippage or
posterior (back) slippage of one vertebra on another following bilateral
fracture of the pars interarticularis. The slippage is graded from 1-4 (25% to
100%) from an x-ray. In degenerative spondylolisthesis, as the intervertebral
disc loses height, the annulus may bulge circumferentially and the ligamentum
flavum can buckle. These types of injuries are seen in wrestlers, due to the
combined extension and rotation movements seen in the sport as well as in older
patients due to their lifestyle. Physical therapy/training emphasis is on elimination of extension-based
exercise (back extension, press-ups, etc.). Biomechanically, this will force
the vertebra forward causing more translation and instability. Training emphasis is on flexion-based exercises (strengthening of
abdominals). Flexion based exercises will decrease shearing force and
translation on the effected segment. Postural education is key, static and
dynamic core strengthening should also be included. Core strengthening using medicine balls, cables and physio balls shoulder
be personalized to the client.
Recommendations
All of the spinal conditions discussed
previously are unique, requiring a thorough understanding, while designing a
program that is personalized for the client. With respect to spondylosis, the
three top exercises for this client are:
Abdominal
bracing with alternate leg lift (as seen in Fig. 1)
 |
| Fig. 1 |
Bridging
with physioball (as seen in Fig 2)
 |
| Fig 2 |
 |
| Fig 3 |
All
three exercises target the multifidus and transverse abdominis; two essential
muscles of the core.
With respect to both
spinal stenosis and spondylolisthesis, the focus is on flexion exercises.
My top three for both include:
Reverse
abdominal crunch (as seen in Fig 4)
 |
| Fig 4 |
Dead bug (as seen in Fig 5)
 |
| Fig 5 |
Prone
alternate leg and arm lift over physioball, stopping at neutral (as seen in Fig 6)
 |
| Fig 6 |
Summary
Lumbar
Spondylosis, Spinal stenosis, and Spondylolisthesis are three common spinal
conditions affecting most adults today. Understanding the pathophysiology,
mechanism of injury, common physical therapy treatments, and a few targeted
exercises, should help you, the fitness professional while designing a program
for your client. If you should have any questions, please feel free to contact
PTCS at ptcg1999@verizon.net
or visit our web site at www.pinnacle-tcs.com.
Wednesday, May 6, 2020
By Chris Gellert, PT, MMusc & Sportsphysio, MPT, CSCS, C-IASTM
There are a multitude of assessments at the fingertips of a fitness professional. Choosing the most accurate and objective assessments should be the cornerstone of any fitness assessment. 3 that we recommend starting with are, the plank, the side plank and the Multifidus Test. These 3 tests are MUST HAVES in your fitness arsenal.
Planking
The plank is an isometric core strength exercise that involves maintaining a position similar to a push-up for the maximum possible time.
 |
Figure 1
|
 |
Figure 2
|
The four-point plank test (Fig. 1) challenges the erector spinae and paraspinal muscles
While the side plank test (Fig 2) challenges the obliques and
quadratus lumborum muscles.
Grading for both tests is as follows:
Normal: Able to lift pelvis off and hold straight 15-20 second count.
Good: Able to lift pelvis off but has difficulty holding spine straight for 15-20 seconds.
Fair: Able to lift pelvis off but has difficulty holding spine straight for 10-15 seconds.
Poor: Able to lift pelvis off but cannot hold for 1-10 seconds.
Trace: Unable to lift pelvis
Multifidus Test
This test assesses the client’s ability or inability to properly contract the multifidi. Have the client lie prone, then palpate multifidi muscle which is ~1” above ilium. Provide instructions asking the client to extend their hip 1-2” off the table and observe what muscles the client elicits.

Normal Movement (Figure 3):
To teach the client to contract the multifidi first, palpate the muscle (figure 1) (instruct the client to perform an anterior pelvic tilt (which shortens and contracts the multifidi), and then have them lift one leg straight up into the air.
 |
Figure 3
Abnormal Movement (Figure 4):
Common compensatory movement is to activate the glutes or hamstrings first, then contract the lower back (this is dysfunctional) as seen in figure 4.
|

As we stated above these are 3 techniques that we strongly recommend but there is a multitude of core assessment tests to choose from. Choose those that are client-specific, safe as well as personalized to the client. In the next article, we will talk about common lumbar conditions..
Monday, May 4, 2020

#SafeExercise #PinnacleTrainingConsultingSystems #PTCS
#LowTrapStrengthening
www.PersonalTrainerCEU.com 443-528-0527
Low Trap Strengthing
• Seated mid-row, one arm DB row, seated reverse flyes (posterior deltoid)
• External rotation with cable/tubing, seated reverse flyes, seated dumbbell side raises (once medically cleared and at least 4 months tissue healing)
• Tricep press downs and barbell bicep curls
• Core strengthening exercises that are safe include; standing trunk rotation with cable/tubing, diagonal with cable tandem in place lunge, planks, planks with a ball, trunk rotation with a forward lunge.
Exercises that are contraindicated include with rationale:
• Seated dumbbell shoulder press (creates excessive load to the medial deltoid).
• Lat pull-downs behind the head (at end or range places the greatest stress on all glenohumeral ligaments as well as on the labrum).
• Barbell squats (places compressive and loading forces on the surgical graft.
• Upright row (at end of range-shoulder is maximally internally rotated which places stress on all glenohumeral ligaments, labrum, and connective tissue).
• Supine dumbbell pullovers (places greatest stress on the anterior capsule and joint).
Subscribe to:
Posts (Atom)